Musculoskeletal Syndrome of Menopause (Wait, what?!)
What do “frozen shoulder” and hip “bursitis” or outer hip pain have in common? They are most common in mid-life women! And, no surprise, they are related to the plummet of Estrogen at perimenopause / menopause either naturally or due to cancer treatments.
>> FAST FACTS:
- 70% of all midlife women will experience musculoskeletal syndrome of menopause.
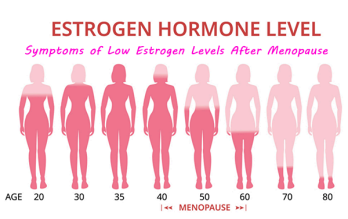
- Most women reach the menopause transition between ages 45 and 55. Symptoms can last up to 10 years!
- This syndrome includes:
- Muscle Pain
- Joint Pain
- Loss of Muscle
- 0.6% loss of muscle mass per year after menopause
- Loss of bone density (hello fractures)
- 10% average reduction after menopause
Tendon and Ligament Injury
Arthritis
- Orthopedic surgeons are often the first point of contact.
It may not be on their radar that midlife hormone changes are likely influencing your condition. This information is still relatively new!
Consider bringing them a copy of this article: Musculoskeletal Syndrome of Menopause.
- Women on MRT (menopausal hormone therapy) are protected against the loss of power (think jump height).
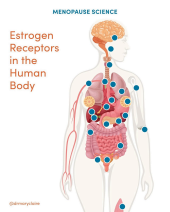
The fall in estrogen levels leads to five main changes:
1. Inflammation
>> Joint pain, muscle damage
2. Reduced muscle mass and strength
3. Reduced muscle regeneration and recovery after injury
4. Osteoarthritis (joint pain and stiffness)
5. Osteoporosis
>> Often under-diagnosed, preventable, and treatable.
>> 30-50% of women suffer a fracture in their life and 70% of hip fractures occur in women.
>> Osteoporotic fractures are extremely detrimental since they can lead to chronic pain, deformity, disability and even death.
Updated Guidelines and Clinical Management:
▪ Conservative approaches include testing, nutrition, and exercise.
>> Testing: Osteoporosis screening is recommended for women aged 65 or older and for those 50-64 who have certain risk factors, including positive family history of osteoporosis.
▪ Women who are treated with aromatase inhibitors or Tamoxifen, or
otherwise have premature ovarian insufficiency are encouraged to discuss osteoporosis screening with their treatment team.
>> Nutrition:

▪ Good quality, bio-available protein is at the top of the list at each meal. ▪ Eating a rainbow of vegetables and fruits, mostly vegetables.
▪ Vitamin D supplementation for improved hip bone mineral density.
▪ Magnesium supplementation significantly increases Vitamin D levels.
▪ Vitamin K2 supplementation has shown significant increases of bone mineral density.
▪ Creatine in tandem with resistance training has shown positive bone mineral density and muscle power improvement.
The good news –
>> EXERCISE:
The one intervention that is unanimously supported in the literature to counter the effects of aging and decline in hormones!



>> EXERCISE is the one intervention that is unanimously supported in the literature to counter the effects of aging and decline in hormones.
Guidelines for optimal weight training in perimenopause and menopause are still lacking, but here are the most current guidelines:
▪ Heavier weights and lower repetition training (2 x 10 reps).
▪ Resistance training or High Intensity Interval Training (HIIT) can better address weight loss resistance, especially around our mid-sections.
If you are a woman in perimenopause or menopause, either naturally occurring or due to surgery or cancer-related treatments, you may need to educate your primary care physician about the physiological effects of estrogen on the musculoskeletal system. This is relatively new science, and it is not something that your physician or other healthcare provider likely received in their medical training.
*** You do not need to accept “It’s time to start slowing down” or “this tends to happen as women age”.
The Musculoskeletal Syndrome of Menopause is a new term to describe the symptoms related to loss of estrogen levels on BONES, MUSCLES, and JOINTS.
Treatment with proper nutrition, vitamin intake, resistance training and (if appropriate) MHT (menopausal hormone therapy) affect quality of life, fall prevention, and reduced frailty and mortality.
Additional Lifestyle Strategies to optimize overall health during this transition and beyond:
1. Sleep: 7-9 hours every day.
Less than 5 hours of sleep per night is associated with an increased risk for osteoporosis!
2. Stress Management: Daily mindfulness, meditation, breathing strategies, being out in nature, being with people you love.
3. Getting outside every day into nature / sunlight –
Early morning walks in particular help to reset our circadian rhythms.
4. Daily walks / runs: minimum 20 minutes daily walking (build up to that as needed) 150 minutes of moderate intensity aerobic exercise each week. Dance, swim, bike ride, brisk walk, run… What do you like to do?
For more information and inspiration, click on the link below to check out Dr. Vonda Wright, double-board certified orthopedic surgeon, author, researcher and consultant!
If concerns over leaking urine are interfering with your ability to get started, or you don’t feel secure through your low back and abdominal region,
Heart of Gold Physical Therapy can help!
The initial visit at Heart of Gold PT offers a full hour dedicated to YOU. Together we determine an appropriate treatment plan just for you.
Now FEATURING our advanced rehabilitation ultrasound imaging (the same technology used for pregnant mamas!). Visualize the muscles of your pelvic floor and layers of your abdominal wall and core, to help YOU gain optimal function in these deep muscles and achieve your goals!